Printable Maryland 510 Template
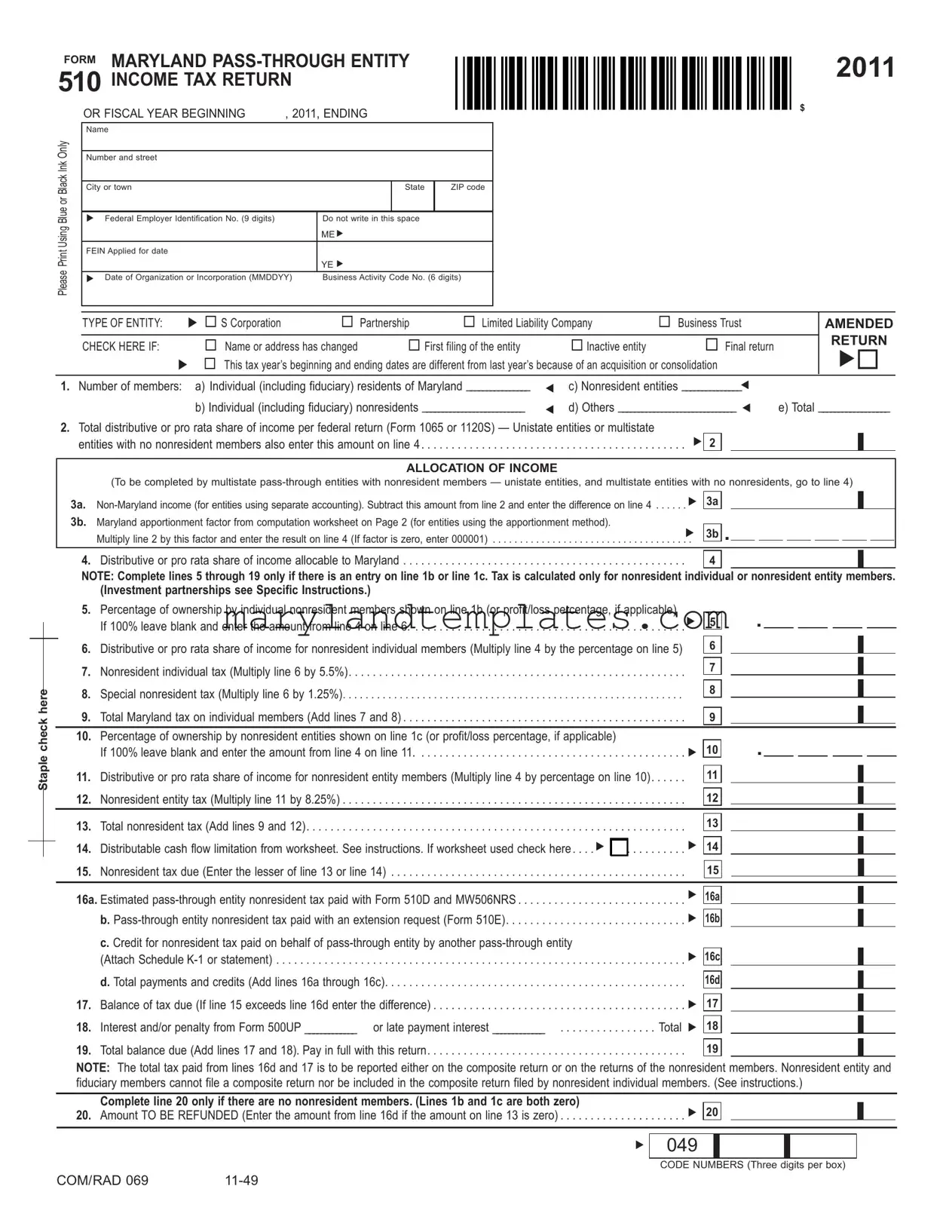
The Maryland Pass-Through Entity 510 Income Tax Return, commonly referred to as Form 510, serves as a critical document for various business entities operating within the state. This form is primarily utilized by S Corporations, partnerships, limited liability companies, and business trusts to report their income and tax obligations. It requires essential information such as the entity's name, address, and Federal Employer Identification Number (FEIN). Entities must indicate their type and provide details regarding their members, including the number of individual residents and nonresidents. Furthermore, Form 510 facilitates the allocation of income, particularly for multistate entities, allowing them to delineate Maryland income from non-Maryland income. Tax calculations are based on distributive shares of income, with specific lines dedicated to nonresident individual and entity members. The form also includes sections for reporting tax payments, credits, and any adjustments required due to IRS changes. In summary, Form 510 is integral for compliance, ensuring that pass-through entities accurately report their income and fulfill their tax responsibilities in Maryland.
Maryland 510 Preview
FORM MARYLAND
|
OR FISCAL YEAR BEGINNING |
, 2011, ENDING |
|
|||
|
Name |
|
|
|
|
|
Only |
|
|
|
|
|
|
Number and street |
|
|
|
|
||
Ink |
|
|
|
|
||
|
|
|
|
|
|
|
Blue or Black |
|
|
|
|
|
|
City or town |
|
|
State |
ZIP code |
||
|
|
|
|
|
|
|
|
Federal Employer Identification No. (9 digits) |
|
Do not write in this space |
|
||
Using |
|
|
|
ME |
|
|
|
|
|
|
|
||
FEIN Applied for date |
|
|
|
|
||
|
|
|
YE |
|
||
Please |
|
|
|
|
|
|
|
Date of Organization or Incorporation (MMDDYY) |
Business Activity Code No. (6 digits) |
||||
|
|
|
|
|
|
|
2011
$
Staple check here
|
TYPE OF ENTITY: |
S Corporation |
Partnership |
Limited Liability Company |
Business Trust |
|
AMENDED |
|||
|
|
|
|
|
|
|
|
RETURN |
||
|
CHECK HERE IF: |
Name or address has changed |
First filing of the entity |
|
Inactive entity |
Final return |
|
|||
|
This tax year’s beginning and ending dates are different from last year’s because of an acquisition or consolidation |
|
|
|||||||
1. Number of members: |
a) Individual (including fiduciary) residents of Maryland ________________ |
|
c) Nonresident entities _______________ |
|
|
|||||
|
|
b) Individual (including fiduciary) nonresidents __________________________ |
|
d) Others ______________________________ |
e) Total __________________ |
|||||
2.Total distributive or pro rata share of income per federal return (Form 1065 or 1120S) — Unistate entities or multistate
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .entities with no nonresident members also enter this amount on line 4 |
|
2 |
ALLOCATION OF INCOME
(To be completed by multistate
3a.
Multiply line 2 by this factor and enter the result on line 4 (If factor is zero, enter 000001) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 3b .
4. Distributive or pro rata share of income allocable to Maryland |
4 |
NOTE: Complete lines 5 through 19 only if there is an entry on line 1b or line 1c. Tax is calculated only for nonresident individual or nonresident entity members.
(Investment partnerships see Specific Instructions.)
5. |
Percentage of ownership by individual nonresident members shown on line 1b (or profit/loss percentage, if applicable) |
|
|
|
. |
|
|
|
|
|
|
|
|||||||
|
If 100% leave blank and enter the amount from line 4 on line 6 |
. . . |
. . |
. |
. . . . . . . . . |
5 |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Distributive or pro rata share of income for nonresident individual members (Multiply line 4 by the percentage on line 5) |
|
|
6 |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Nonresident individual tax (Multiply line 6 by 5.5%) |
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
. . . |
. . |
. |
. . . . . . . . . |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
8. |
Special nonresident tax (Multiply line 6 by 1.25%) |
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
. . . |
. |
. . . . . . . . . |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
9. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total Maryland tax on individual members (Add lines 7 and 8) |
. . . |
. . |
. |
. . . . . . . . . |
|
|
9 |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. |
Percentage of ownership by nonresident entities shown on line 1c (or profit/loss percentage, if applicable) |
|
|
|
|
. |
|
|
|
|
|
|
|
||||||
|
If 100% leave blank and enter the amount from line 4 on line 11 |
. . . |
. . |
. |
. . . . . . . . . |
|
|
10 |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. |
Distributive or pro rata share of income for nonresident entity members (Multiply line 4 by percentage on line 10) |
|
|
11 |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. |
Nonresident entity tax (Multiply line 11 by 8.25%) |
. . . |
. . |
. |
. . . . . . . . . |
|
|
12 |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. |
Total nonresident tax (Add lines 9 and 12) |
. . . |
. . |
. |
. . . . . . . . . |
|
|
13 |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. |
Distributable cash flow limitation from worksheet. See instructions. If worksheet used check here |
|
|
|
|
|
|
14 |
|
|
|
|
|
|
|
|
|
||
. . . |
. . |
. |
. . . . . . . . . |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. |
Nonresident tax due (Enter the lesser of line 13 or line 14) |
. . . |
. . |
. |
. . . . . . . . . |
|
|
|
15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16a. Estimated
b.
|
c. Credit for nonresident tax paid on behalf of |
|
|
(Attach Schedule |
. . . . . 16c |
|
d. Total payments and credits (Add lines 16a through 16c) |
. . . . . 16d |
17. |
Balance of tax due (If line 15 exceeds line 16d enter the difference) |
. . . . . 17 |
18. |
Interest and/or penalty from Form 500UP _____________ or late payment interest _____________ |
Total 18 |
19. |
Total balance due (Add lines 17 and 18). Pay in full with this return |
. . . . . 19 |
NOTE: The total tax paid from lines 16d and 17 is to be reported either on the composite return or on the returns of the nonresident members. Nonresident entity and fiduciary members cannot file a composite return nor be included in the composite return filed by nonresident individual members. (See instructions.)
Complete line 20 only if there are no nonresident members. (Lines 1b and 1c are both zero)
20. Amount TO BE REFUNDED (Enter the amount from line 16d if the amount on line 13 is zero) . . . . . . . . . . . . . . . . . . . . . 20
049
CODE NUMBERS (Three digits per box)
COM/RAD 069 |
FORM MARYLAND
2011
NAME __________________________ FEIN ___________________________
Page 2
SCHEDULE A – |
|
Column 1 |
Column 2 |
|
|
|
|
|
Column 3 |
|
|
||||||||||
|
TOTALS |
TOTALS |
|
|
|
DECIMAL FACTOR |
|
|
|||||||||||||
COMPUTATION OF APPORTIONMENT FACTOR |
|
|
|
|
|
||||||||||||||||
(Applies only to multistate |
WITHIN |
WITHIN AND |
|
|
Column 1 ÷ Column 2 |
|
|
||||||||||||||
MARYLAND |
WITHOUT |
( rounded to six places |
) |
|
|||||||||||||||||
NOTE: Special apportionment formulas are required for rental/leasing, transportation, financial |
|
||||||||||||||||||||
|
institutions and manufacturing companies. See Instructions. |
|
MARYLAND |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1A. |
Receipts |
a. Gross receipts or sales less returns and allowances |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Dividends |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .c. Interest |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. Gross rents |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e. Gross royalties |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f. |
Capital gain net income |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .g. Other income (Attach schedule) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
h. Total receipts (Add lines 1A(a) through 1A(g), for Columns 1 and 2) . |
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
1B. |
Receipts |
Enter the same factor shown on line 1A, Column 3. Disregard this line |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
if special apportionment formula used |
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Property |
a. Inventory |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .b. Machinery and equipment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .c. Buildings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .d. Land |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. . . . . . . . . . . . . . . . . . . . . . . .e. Other tangible assets (Attach schedule) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. . . . . . . . . . . . . . . . . . .f. Rent expense capitalized (Multiplied by eight) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. . . . . .g. Total property (Add lines 2a through 2f, for Columns 1 and 2) |
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Payroll |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .a. Compensation of officers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .b. Other salaries and wages |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. . . . . . . . . .c. Total payroll (Add lines 3a and 3b, for Columns 1 and 2) |
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Total of factors (Add entries in Column 3) |
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
5.Maryland apportionment factor Divide line 4 by four for
formula required (If factor is zero, enter 000001 on line 3b, Page 1.) |
|
. |
|
ADDITIONAL INFORMATION REQUIRED
1.Address of principal place of business (if other than indicated on page 1):
2.Address at which tax records are located (if other than indicated on page 1):
3.Telephone number of
4.State of organization or incorporation:
5.Has the Internal Revenue Service made adjustments (for a tax year in which a Maryland return was required) that were not previously reported to the
|
Maryland Revenue Administration Division? |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
Yes |
No |
|
|
If “yes”, indicate tax year(s) here: |
|
and submit an amended return(s) together with a copy of the IRS adjustment report(s) under |
||
|
separate cover. |
|
|
|
|
6. |
Did the |
► Yes |
No |
||
7. |
Is this entity a multistate corporation that is a member of a unitary group?. . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
► Yes |
No |
|
8. |
Is this entity a multistate manufacturing corporation with more than 25 employees? If so, complete and attach Form 500MC to your Form 510 |
► Yes |
No |
||
SIGNATURE AND VERIFICATION: Under penalties of perjury, I declare that I have examined this return (including attachments) and, to the best of my knowledge and belief, it is true, correct and
complete. (Declaration of preparer other than the taxpayer is based on all information of which preparer has any knowledge.) Check here 
 if you authorize your preparer to discuss this return with us.
if you authorize your preparer to discuss this return with us.
|
|
|
|
|
|
|
|
Signature of general partner, officer or member |
|
Date |
Preparer’s SSN or PTIN (required by law) |
Preparer’s signature |
|
||
|
|
|
|
|
|
|
|
Title |
|
|
Preparer’s name, address and telephone number |
|
|||
Make checks payable and mail to:
Comptroller of Maryland, Revenue Administration Division 110 Carroll Street
Annapolis, Maryland
(Write federal employer identification number on check)
COM/RAD 069 |
SCHEDULE B |
MARYLAND |
2011 |
FORM 510 |
|
|
|
MEMBERS’ INFORMATION |
|
Name shown on Form 510
Federal employer identification number (9 digits)
PART I – INDIVIDUAL MEMBERS’ INFORMATION
Enter the Information in Social Security Number Order
|
|
Check |
|
|
|
|
|
here if |
Distributive or pro |
Distributive or pro |
Distributive or pro |
Social Security Number and name of member |
Address |
Maryland: |
rata share of income |
rata of tax paid |
rata share of tax credit |
|
|
|
(See Instructions) |
(See Instructions) |
(See Instructions) |
|
|
Non- |
|||
|
|
|
|
|
|
|
|
Resident Resident |
|
|
|
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
SUBTOTAL from additional Form 510 Schedule B for individual members
TOTAL:
SCHEDULE B |
MARYLAND |
2011 |
FORM 510 |
|
|
|
MEMBERS’ INFORMATION |
|
Name shown on Form 510
Federal employer identification number (9 digits)
PART II – FIDUCIARY MEMBERS’ INFORMATION
Enter the Information in Federal Employer Identification Number Order
|
|
Check |
|
|
|
|
Federal employer identiication number and name |
|
here if |
Distributive or pro |
Distributive or pro |
Distributive or pro |
|
Address |
Maryland: |
rata share of income |
rata of tax paid |
rata share of tax credit |
||
of estate or trust |
||||||
|
|
(See Instructions) |
(See Instructions) |
(See Instructions) |
||
|
|
Non- |
||||
|
|
|
|
|
||
|
|
Resident Resident |
|
|
|
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
SUBTOTAL from additional Form 510 Schedule B for iduciary members
TOTAL:
SCHEDULE B |
MARYLAND |
2011 |
FORM 510 |
|
|
|
MEMBERS’ INFORMATION |
|
Name shown on Form 510
Federal employer identification number (9 digits)
PART III –
Enter the Information in Federal Employer Identification Number Order
|
|
Is Member a |
Distributive or |
Distributive or pro |
Distributive or pro |
|
Federal employer identification number |
|
Nonresident |
pro rata share of |
rata share of tax |
||
Address |
Entity: |
rata of tax paid |
||||
and name of |
income |
credit |
||||
|
|
(See Instructions) |
||||
|
|
YES NO |
(See Instructions) |
(See Instructions) |
||
|
|
|
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
SUBTOTAL from additional Form 510 Schedule B for PTE members
TOTAL:
SCHEDULE B |
MARYLAND |
2011 |
FORM 510 |
|
MEMBERS’ INFORMATION
Name shown on Form 510
Federal employer identification number (9 digits)
PART IV – CORPORATION MEMBERS’ INFORMATION (EXCLUDING S CORPORATIONS)
Enter the Information in Federal Employer Identification Number Order
|
|
Is Member a |
Distributive or |
Distributive or pro |
Distributive or pro |
|
Federal employer identification number |
|
Nonresident |
pro rata share of |
rata share of tax |
||
Address |
Entity: |
rata of tax paid |
||||
and name of |
income |
credit |
||||
|
|
(See Instructions) |
||||
|
|
YES NO |
(See Instructions) |
(See Instructions) |
||
|
|
|
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
SUBTOTAL from additional Form 510 Schedule B for corporate members
TOTAL:
Form Attributes
| Fact Name | Detail |
|---|---|
| Purpose | The Maryland 510 form is used for reporting income tax for pass-through entities, such as S corporations, partnerships, and limited liability companies. |
| Filing Requirements | Entities must file the Maryland 510 if they have income that is allocable to Maryland, regardless of their residency status. |
| Governing Laws | This form is governed by Maryland tax law, specifically under Title 10 of the Tax-General Article. |
| Important Dates | The form must be filed annually, with deadlines typically aligned with the federal tax return due dates. |
Other PDF Forms
Maryland Dc 70 - By filling out this form, the requester acknowledges their responsibility to inform all parties affected by the potential delay.
Maryland Annual Report 2023 - Form 4A categorizes assets into current assets, property, plant, and equipment, and intangible and other assets for a comprehensive financial snapshot.
When transferring ownership of your vehicle, the importance of a comprehensive document cannot be overstated. The Washington Motor Vehicle Bill of Sale provides all necessary details to solidify the transaction, making sure both parties have a clear record. To facilitate this process and avoid any ambiguities, it's recommended to carefully complete the form, which you can access through WA Documents.
Motion for Modification of Sentence - Filing option available for Maryland defendants convicted of certain offenses to seek modifications for treatment purposes.