Printable Maryland Confidential Morbidity Report Template
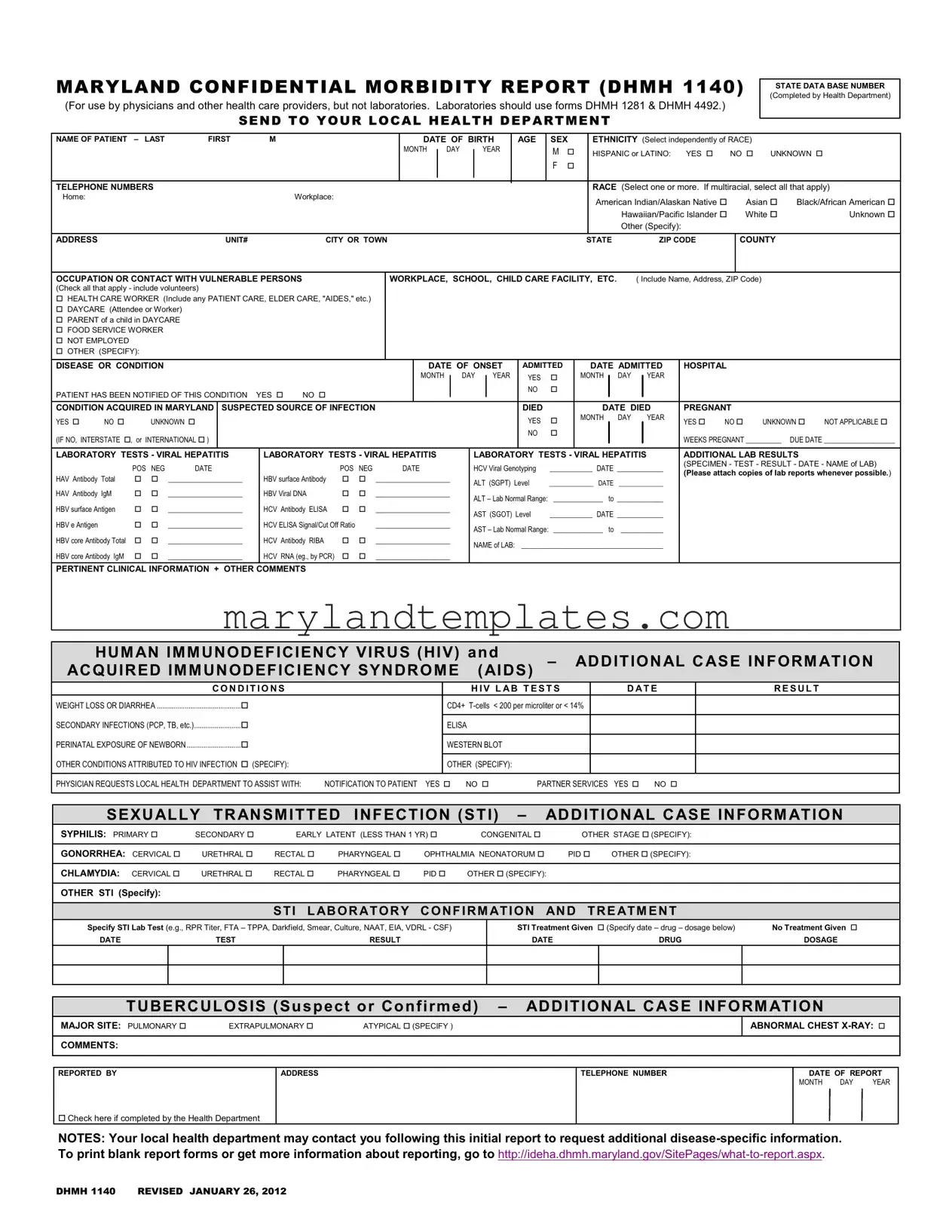
The Maryland Confidential Morbidity Report form, designated as DHMH 1140, serves a crucial role in the public health landscape by enabling healthcare providers to report specific diseases and conditions to local health departments. This form is primarily utilized by physicians and other healthcare professionals, excluding laboratories, which have their own designated reporting forms. Essential details required on the form include patient demographics such as name, date of birth, sex, ethnicity, and contact information. Furthermore, it captures vital occupational information, particularly regarding interactions with vulnerable populations. The form also necessitates the documentation of the disease or condition, including onset dates, hospital admission details, and any relevant laboratory test results. The reporting process is designed to maintain patient confidentiality while facilitating timely public health responses. Additional sections address conditions related to sexually transmitted infections, tuberculosis, and HIV/AIDS, allowing for comprehensive data collection. Notably, the form emphasizes the importance of notifying patients and offers a mechanism for local health departments to assist in partner services and further patient outreach. This structured approach not only aids in disease tracking but also enhances the overall health response within the state.
Maryland Confidential Morbidity Report Preview
MARYLAND CONFIDENTIAL MORBIDITY REPORT (DHMH 1140)
(For use by physicians and other health care providers, but not laboratories. Laboratories should use forms DHMH 1281 & DHMH 4492.)
SEND TO YOUR LOCAL HEALTH DEPARTMENT
STATE DATA BASE NUMBER (Completed by Health Department)
NAME OF PATIENT |
– LAST |
FIRST |
|
M |
|
|
|
|
|
|
DATE OF BIRTH |
|
AGE |
SEX |
|
ETHNICITY (Select independently of RACE) |
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
DAY |
|
|
YEAR |
|
|
M |
|
|
HISPANIC or LATINO: |
YES |
|
NO |
UNKNOWN |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE NUMBERS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RACE (Select one or more. If multiracial, select all that apply) |
|||||||||||||||||
Home: |
|
|
|
|
|
|
|
Workplace: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
American Indian/Alaskan Native |
|
Asian |
Black/African American |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hawaiian/Pacific Islander |
|
White |
|
Unknown |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify): |
|
|
|
|
|
|
|
|||
ADDRESS |
|
|
|
|
UNIT# |
|
|
CITY OR TOWN |
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP CODE |
|
|
COUNTY |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
OCCUPATION OR CONTACT WITH VULNERABLE PERSONS |
|
|
|
WORKPLACE, SCHOOL, CHILD CARE FACILITY, ETC. |
|
( Include Name, Address, ZIP Code) |
|
|
|
|||||||||||||||||||||||||||||||||
(Check all that apply - include volunteers) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
HEALTH CARE WORKER (Include any PATIENT CARE, ELDER CARE, "AIDES," etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
DAYCARE (Attendee or Worker) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
PARENT of a child in DAYCARE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
FOOD SERVICE WORKER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
NOT EMPLOYED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
DISEASE OR CONDITION |
|
|
|
|
|
|
|
|
|
|
DATE OF ONSET |
ADMITTED |
|
|
DATE ADMITTED |
|
HOSPITAL |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
|
DAY |
|
YEAR |
YES |
|
|
MONTH |
|
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
PATIENT HAS BEEN NOTIFIED OF THIS CONDITION |
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
CONDITION ACQUIRED IN MARYLAND |
SUSPECTED SOURCE OF INFECTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
DIED |
|
|
|
|
DATE DIED |
|
PREGNANT |
|
|
|
|||||||||||||||||
YES |
NO |
|
UNKNOWN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
MONTH |
DAY |
|
YEAR |
|
YES |
NO |
UNKNOWN |
NOT APPLICABLE |
||||||||
(IF NO, INTERSTATE , or INTERNATIONAL ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
WEEKS PREGNANT __________ |
DUE DATE ____________________ |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
|
|
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
ADDITIONAL LAB RESULTS |
|
||||||||||||||||||||||||||||||||
|
|
POS |
NEG |
DATE |
|
|
|
POS |
NEG |
|
|
DATE |
|
|
|
|
HCV Viral Genotyping |
____________ |
DATE _____________ |
|
(SPECIMEN - TEST - RESULT - DATE - NAME of LAB) |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
(Please attach copies of lab reports whenever possible.) |
||||||||||||||||||||||||||||||
HAV Antibody Total |
|
|
_____________________ |
|
HBV surface Antibody |
|
|
_____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
ALT (SGPT) Level |
______________ |
DATE |
______________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HAV Antibody IgM |
|
|
_____________________ |
|
HBV Viral DNA |
|
|
_____________________ |
|
|
|
ALT – Lab Normal Range: |
______________ to _____________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV surface Antigen |
|
|
_____________________ |
|
HCV Antibody ELISA |
|
|
_____________________ |
|
|
|
AST (SGOT) Level |
____________ |
DATE _____________ |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV e Antigen |
|
|
|
_____________________ |
|
HCV ELISA Signal/Cut Off Ratio |
|
_____________________ |
|
|
|
AST – Lab Normal Range: ______________ to |
____________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV core Antibody Total |
|
|
_____________________ |
|
HCV Antibody RIBA |
|
|
_____________________ |
|
|
|
NAME of LAB: |
________________________________________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV core Antibody IgM |
|
|
_____________________ |
|
HCV RNA (eg., by PCR) |
|
|
_____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
PERTINENT CLINICAL INFORMATION + OTHER COMMENTS
|
HUMAN IMMUNODEFICIENCY VIRUS (HIV) and |
– |
ADDITIONAL CASE INFORMATION |
||||
|
ACQUIRED IMMUNODEFICIENCY SYNDROME |
(AIDS) |
|||||
|
CON D IT IO NS |
|
H IV L AB T EST S |
|
D AT E |
RESULT |
|
|
WEIGHT LOSS OR DIARRHEA ............................................. |
CD4+ |
|
|
|||
|
SECONDARY INFECTIONS (PCP, TB, etc.)......................... |
|
|
|
|
|
|
|
ELISA |
|
|
|
|
|
|
|
PERINATAL EXPOSURE OF NEWBORN ............................. |
|
|
|
|
|
|
|
WESTERN BLOT |
|
|
|
|
||
|
OTHER CONDITIONS ATTRIBUTED TO HIV INFECTION (SPECIFY): |
|
|
|
|
|
|
|
OTHER (SPECIFY): |
|
|
|
|
||
PHYSICIAN REQUESTS LOCAL HEALTH DEPARTMENT TO ASSIST WITH: NOTIFICATION TO PATIENT YES NO PARTNER SERVICES YES NO
SEXUALLY TRANSMITTED INFECTION (STI) – |
ADDITIONAL CASE INFORMATION |
|||||
SYPHILIS: PRIMARY |
SECONDARY |
EARLY LATENT (LESS THAN 1 YR) |
CONGENITAL |
OTHER STAGE (SPECIFY): |
||
|
|
|
|
|
|
|
GONORRHEA: CERVICAL |
URETHRAL |
RECTAL |
PHARYNGEAL |
OPHTHALMIA NEONATORUM |
PID OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
CHLAMYDIA: CERVICAL |
URETHRAL |
RECTAL |
PHARYNGEAL |
PID |
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
OTHER STI (Specify): |
|
|
|
|
|
|
STI LABORATORY CONFIRMATION AND TREATMENT
Specify STI Lab Test (e.g., RPR Titer, FTA – TPPA, Darkfield, Smear, Culture, NAAT, EIA, VDRL - CSF)
DATE |
TEST |
RESULT |
STI Treatment Given (Specify date – drug – dosage below) |
No Treatment Given |
|
DATE |
DRUG |
DOSAGE |
TUBERCULOSIS (Suspect or Confirmed) – ADDITIONAL CASE INFORMATION
MAJOR SITE: PULMONARY |
EXTRAPULMONARY |
ATYPICAL (SPECIFY ) |
ABNORMAL CHEST
COMMENTS:
REPORTED BY
ADDRESS
TELEPHONE NUMBER
DATE OF REPORT
MONTH DAY YEAR
Check here if completed by the Health Department
NOTES: Your local health department may contact you following this initial report to request additional
DHMH 1140 REVISED JANUARY 26, 2012
Form Attributes
| Fact Name | Details |
|---|---|
| Purpose | The Maryland Confidential Morbidity Report is used by healthcare providers to report certain diseases and conditions. |
| Governing Law | This report is governed by Maryland Health-General Article, § 18-201. |
| Exclusions | Laboratories must use forms DHMH 1281 and DHMH 4492 instead of this report. |
| Patient Information | It requires detailed patient information, including name, date of birth, and ethnicity. |
| Health Department Role | The local health department assigns a state data base number upon receiving the report. |
| Notification Requirement | Providers must indicate whether the patient has been notified of their condition. |
| Pregnancy Status | Providers must report if the patient is pregnant and include details about the pregnancy. |
| Laboratory Tests | The form includes sections for reporting laboratory test results related to viral hepatitis and HIV. |
| Follow-Up | Health departments may contact providers for additional disease-specific information after the initial report. |
Other PDF Forms
Maryland Speeding Ticket - Remember, your Maryland Civil Citation's number, found under the barcode, is the key to addressing your case correctly.
Maryland Annual Report 2023 - Detailing equity components on Form 4A sheds light on a business's funding structure and how it sustains operations and growth.
The California Small Estate Affidavit form is a valuable resource for individuals navigating the estate distribution process. By utilizing the Small Estate Affidavit form, heirs or beneficiaries can more easily claim their assets without the burden of lengthy probate interventions, ensuring a swifter resolution to estate matters.
University of Maryland Application Portal - Only individuals 16 years and older can apply for voluntary admission as per Maryland law.