Printable Maryland Continuation Election Template
The Maryland Continuation Election form is an important document for individuals looking to maintain their health benefits after a qualifying event, such as job loss, divorce, or the death of a spouse. This form allows you to elect to continue your coverage under your employer's Employee Benefit Plan. It’s crucial to understand that this election is bound by the specific terms of the Plan. Before making your decision, you must read the Maryland Continuation Coverage Notice and any accompanying letters. These documents outline your rights and limitations regarding continuation coverage. The form requires you to indicate whether you wish to continue your coverage, and if so, to provide details about your insurance selections, including health, dental, and vision options. You must also specify the type of coverage you desire, such as individual or family plans. Remember, dependents can only be added during open enrollment unless there is a change in family status. Additionally, the form asks for your signature, the date, and your Social Security number, ensuring that all necessary information is accurately captured. If you are submitting your first payment with the form, it is essential, as failing to do so may delay your access to health care coverage. Lastly, your employer will need to complete certain sections, including the end date of your continuation coverage and billing details.
Maryland Continuation Election Preview
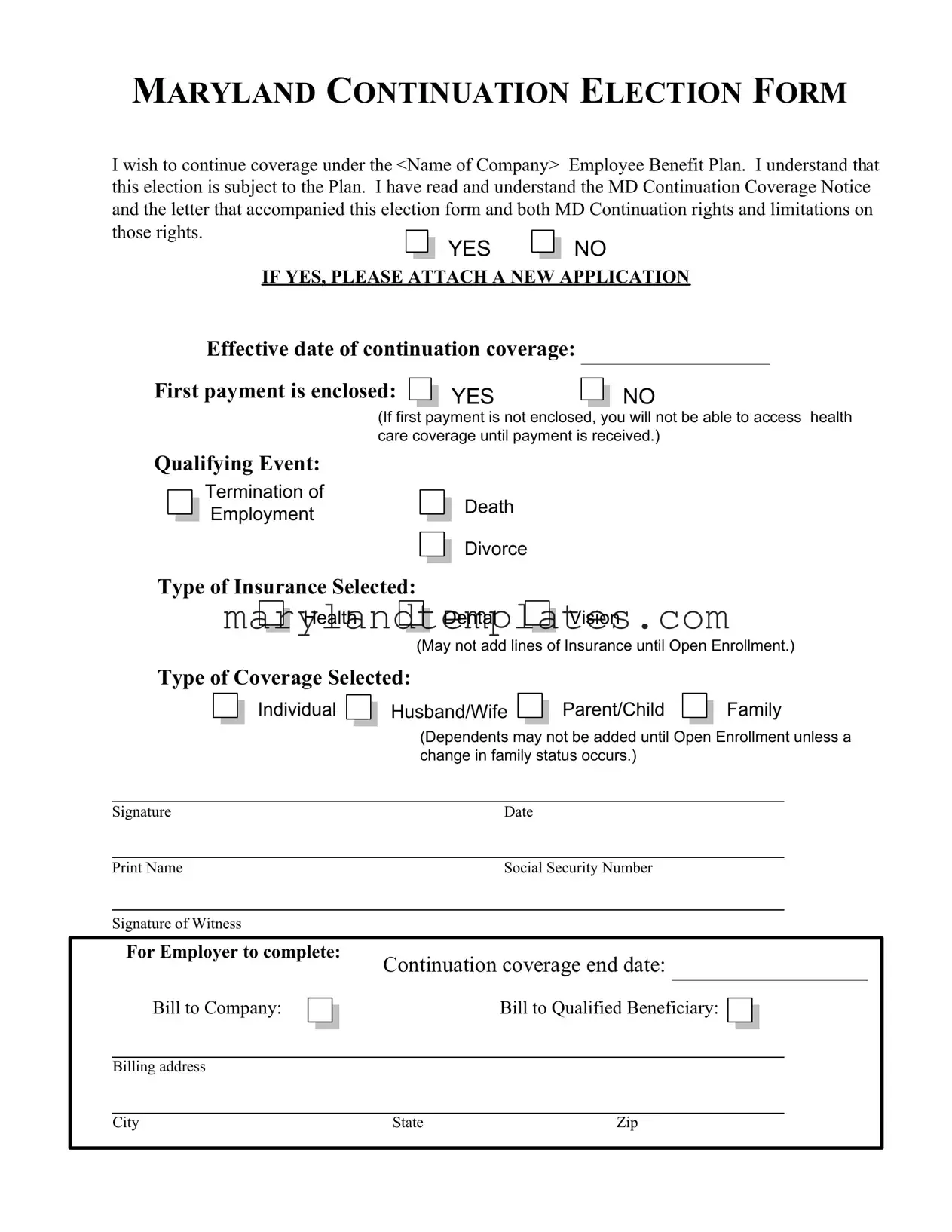
MARYLAND CONTINUATION ELECTION FORM
I wish to continue coverage under the <Name of Company> Employee Benefit Plan. I understand that this election is subject to the Plan. I have read and understand the MD Continuation Coverage Notice and the letter that accompanied this election form and both MD Continuation rights and limitations on those rights.
YES NO
IF YES, PLEASE ATTACH A NEW APPLICATION
Effective date of continuation coverage: |
|
|
First payment is enclosed: |
YES |
NO |
|
||
(If first payment is not enclosed, you will not be able to access health care coverage until payment is received.)
Qualifying Event:
Termination of  Employment
Employment
Death
Divorce
Type of Insurance Selected:

 Health
Health
Dental 
 Vision
Vision
(May not add lines of Insurance until Open Enrollment.)
Type of Coverage Selected:
 Individual
Individual 
 Husband/Wife
Husband/Wife  Parent/Child
Parent/Child
Family
|
|
|
|
|
|
(Dependents may not be added until Open Enrollment unless a |
|||||||
|
|
|
|
|
|
change in family status occurs.) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature |
Date |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Print Name |
Social Security Number |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Witness |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
For Employer to complete: |
Continuation coverage end date: |
|||||||||||
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bill to Company: |
|
|
|
|
Bill to Qualified Beneficiary: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Billing address |
|
|
|
|
|
|
|
|
||||
City |
State |
Zip |
Form Attributes
| Fact Name | Description |
|---|---|
| Purpose | The Maryland Continuation Election Form allows eligible individuals to continue their health insurance coverage after certain qualifying events. |
| Governing Law | This form is governed by the Maryland Health Insurance Coverage Continuation Act. |
| Qualifying Events | Individuals can elect continuation coverage due to termination of employment, death, or divorce. |
| Types of Insurance | The form allows for the selection of health, dental, and vision insurance, with restrictions on adding coverage. |
| Effective Date | The effective date of continuation coverage is specified on the form and is crucial for maintaining uninterrupted health care access. |
| Payment Requirement | The first payment must be enclosed with the form; otherwise, access to health care coverage will be delayed. |
| Dependent Coverage | Dependents may not be added to the insurance plan until the Open Enrollment period unless there is a change in family status. |
| Signature Requirement | The form must be signed by the individual electing coverage and a witness, ensuring accountability and verification. |
Other PDF Forms
How to Start a Lab Business - Incorporates a space for indicating whether the CLIA certification covers multiple sites, catering to larger laboratory networks.
To effectively manage your affairs and ensure your preferences are followed, it is essential to fill out a Power of Attorney form. For more information and to access a reliable template, visit WA Documents, where you can find resources to assist you in this important task.
Court Forms - Understanding the necessity of the Intake Sheet for each land transaction in Maryland to comply with property law and ensure accurate record keeping.
Maryland Form 510d - If an FEIN is pending, entities are instructed to denote the application status and date on the form.